1 Introduction
Critical Care Nurses (CCNs), who are members of the interprofessional team in intensive care units (ICUs), provide care to acutely and critically ill patients and their families (1). The ICUs may be a stressful environment not only to patients and families, but to healthcare professionals as well (2). Challenges related to caring for the critically ill patient, e.g. high degree of responsibility, end-of-life issues, ethical problems, and increased demands regarding technical competencies required, have been identified as some of the major work-related stressors for ICU nurses (3,4). A Norwegian report by Seierstad and Eimot (2015) revealed that one of two CCNs stated that it was unlikely that they would still be in the specialty field of critical care in ten years’ time (5). The factors the CCNs pointed out as challenging were night shifts, high efforts/lower rewards, emotional demands, role conflicts, high job demands, and low control at work (5). The CCNs’ intention to leave their jobs is thus influenced by factors related to their working conditions. The Norwegian government therefore wishes to strengthen competence in healthcare and to make targeted efforts to recruit, retain and educate healthcare professionals in order to secure sufficient frontline staff in the future (6).
Psychological and social factors at work describe the factors in work that are applied in social arenas, and which are influenced by individual psychological processes with consequences for job performance and health (7). According to Dallner et al. (7), psychological and social factors include job demands, role expectations, control at work, predictability at work, mastery of work, social interactions, leadership, organizational culture, work centrality, commitment to the organizations, perceptions of group work, and work motivation. Psychological and social factors are all potential contributors to the health and wellbeing of employees such as CCNs working in intensive care units, and contribute to work motivation, and organizational learning and efficiency (8). Based on the Norwegian report (5), this study focused on 1) job demands, 2) control at work, 3) mastery of work, and 4) work motives. The areas cover both psychological and social factors at work.
2 Background
Job demands incorporate as all those occurrences, circumstances, and conditions that require the individual to act or respond (7). There are different types of demands on workers: the increasing amount of work, time pressure, irregular work, high work pace, and the need for quick decisions. According to Karasek and Theorell (9), demands do not create stress by themselves, but the combination of high demands and low control does. 2) Control at work refers to the perceived freedom or ability to exercise control, regulate, direct, and make decisions about one’s work. In work life, control relates to autonomy and participation in planning and decision-making. According to Dallner (10), several findings indicate that job control may be the main critical component in a healthy work environment. 3) Mastery of work refers to the results of individual behavior, for example the experience of producing a successful outcome. 4) Work motives describes or explains why a person behaves or think in a specific way and refers to the strengths of various facets of behavior-inducing factors, which refer to the individual’s orientation towards a job: the realization of one’s potential for self-development and creativeness. Extrinsic motivation to work is associated with certain personal dispositions and expectations, related to the employee’s background (9).
2.1 Literature Review
The literature review was conducted prior to and during the study period and is based on the keywords “critical care nurses,” “job demands,” “psychological and social factors,” and “working conditions.” A study by Berland et al. (11) among CCNs in Norway found that for the CCNs, a workplace with high demands and low control combined with lack of support from colleagues may lead to rapid pace, stress, and impaired health (11). International studies show that sick leave and staff turnover are found to be related to psychological, social, and organizational work factors for nurses working at hospitals (12,13,14). Nurses working at ICUs state that work factors may affect both level of competence and patient safety (15). On the other hand, positive perceptions of psychological and social factors of work are found to be associated with work engagement among healthcare professionals (16,17).
High staff turnover among nursing staff is currently also observed in ICUs in other countries (18,19,20). Research found an inverse relationship between years of experience and intention to leave current job (20). Daouda, Hocine, and Temime (21) found that social support from colleagues as well as long experience in the profession were negatively associated with turnover. High turnover rate may lead to inadequate staffing and higher patient mortality rates (22,23).
Some research has been carried out with regard to burnout and work motivation among CCNs (24), but there has been less focus on requirements and control when it comes to the CCNs’ psychosocial working environment. Research that illuminates CCNs perception of psychological and social factors at work, may lay a basis for quality improvement in CCNs’ working environment, and may reduce the chance of CNNs leaving their jobs. Significant differences in CCNs’ compassion of satisfaction and fatigue based on sex, age, and educational level are reported (25). Since CCNs working in the ICU are of different ages, have varying experiences, and work different shifts, it is of interest to study these specific characteristics in relation to CCNs’ perception of psychological and social factors. Norwegian research in the area of intensive care is sparse, and most studies are international and based on health services that are organized in different ways from the Norwegian health service.
The aim of this study was to investigate critical care nurses’ (CCNs’) perceptions of psychological and social factors at work in an intensive care unit (ICU).
The aim was addressed through the following research questions:
1) How do CCNs perceive job demands, control at work, mastery of work and work motives related to their work in ICUs?
2) Is there any difference between CCNs’ perceptions of job demands, control at work, mastery of work and work motives regarding age, gender, years in present workplace, experience as a CCN and type of working shifts?
3 Methods
3.1 Design
The study used a cross-sectional design, including data collected from CCNs in Norway. The STROBE statement checklist has been provided for reporting the study (Appendix 1).
3.2 Setting and Sample Characteristics
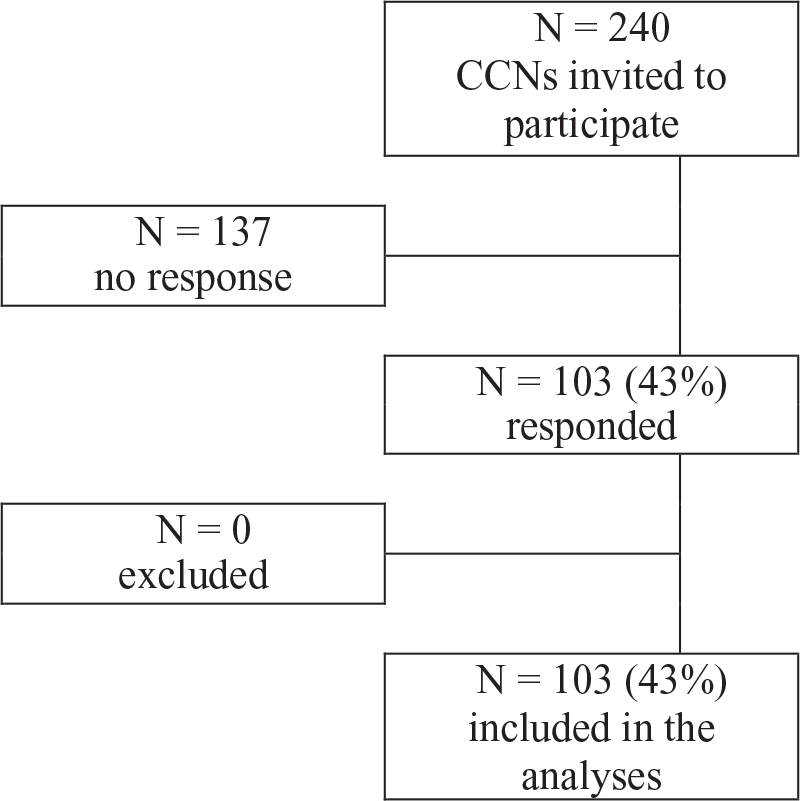
All of the CCNs (n = 240) working in 15 ICUs in four Norwegian hospitals in urban areas were invited to participate in this study. The units were general intensive care units with both surgical and medical patients. The inclusion criteria for participation were being a postgraduate CCN, and at least six months permanent employment in a 50% position or more in their units. Nurse leaders were excluded.
3.3 Questionnaire
The General Nordic Questionnaire for Psychological and Social Factors at Work (QPSNordic) (8) developed by the Nordic Council of Ministers was used. The questionnaire, which is designed for assessment of psychological, social and organizational factors at work, includes 14 areas with 26 scales and 38 single items (8). The four areas Job demands, Control at work, Mastery of work, and Work motives containing nine scales and 12 single items were selected for this study (Table 1). For the areas Job demands, Control at work and Mastery of work, the items used a five-point Likert response scale, rating from “1 = very seldom or never” to “5 = very often or always.” For the area Work motives, the items were rated from “1 = unimportant” to “5 = absolutely necessary.” The Cronbach alpha values for the original questionnaire were between 0.61 and 0.83 for the selected areas. In this study, the Cronbach alpha values were between 0.40 and 0.78 (Table 1). The background questions contained items about age, gender, years in present workplace, experience as a CCN after postgraduation, and type of shifts. The two-shift pattern involves all kind of shifts, except night shift.
| Items | Cronbach’s alpha | |
|---|---|---|
| QPSNordic
Areas and scales used in this study |
32 | 0.66 |
| Job demands
Quantitative demands Decision demands Learning demands |
4 3 3 |
0.55 0.47 0.40 |
| Control at work
Positive challenges at work Control of decisions Control of work pace |
3 5 4 |
0.66 0.61 0.67 |
| Mastery og work
Perception of mastery |
4 |
0.78 |
| Work motives
Intrinsic motivation to work Extrinsic motivation to work |
3 3 |
0.52 0.51 |
3.4 Data Collection
The data collection took place in the course of three weeks in the spring of 2016, during normal working hours excluding annual holidays. The head nurse or her assistant distributed a paper version of the questionnaire to the CCNs. One reminder was sent by email. The CCNs returned the questionnaire anonymously in a sealed envelope, placed in a sealed box at each unit.
3.5 Data Analysis
The IBM SPSS Statistics v. 23 was used for the statistical analysis. Descriptive statistics were conducted to describe the sample characteristics, displaying the frequencies, percentages, means and standard deviations. The Cronbach’s alpha was run to estimate internal consistency for all scales.
Both parametric and non-parametric tests were applied. As the scale scores were based on ordinal data (five-point Likert scale), and the assumptions were met, a one-way analysis of variance (ANOVA) was conducted to compare between the three groups. Tuckey post hoc tests were conducted to identify differences between the groups. A T-test was used to compare between two groups.
Comparisons of single items between groups of three were conducted using a non-parametric Kruskal-Wallis test. A p-value of p < 0,05 was considered as appropriate for all tests.
3.6 Ethics
The study was approved by the Norwegian Social Science Data Services (ref. 47710), and senior management at the hospitals gave their consent. Ethical guidelines for nursing research in the Nordic countries (26) were followed.
The principle of voluntariness was emphasized in the written information about the study. Filling in the form was considered as confirmation of willingness to participate. To ensure anonymity and confidentiality, an anonymized form was used, and no data about the participants’ workplace was given.
4 Results
A total of 103 CCNs (43%) completed the questionnaire (Figure 1). Most of the participants were women in full time employment and working two or three shifts. Additionally, half of the participants were aged between 36–49 years and had worked 6–14 years as a postgraduate CCN (Table 2).
| Groups | Mean (SD) | n (%) | |
|---|---|---|---|
| Gender (n = 103) |
Women Men |
91 (88.3) 12 (11.7) |
|
| Age (n = 102) |
≤ 35 year 36–49 year ≥ 50 year |
45.34 (8.07) |
14 (13.72) 51 (50.00) 37 (36.28) |
| Experience as CCN after postgraduate (n = 100) |
≤ 5 year 6–14 year ≥15 year |
12.15 (7.09) |
17 (17) 50 (50) 33 (33) |
| Years in present workplace (N = 103) |
≤ 5 year 6–14 year ≥ 15 year |
9.29 (6.65) |
39 (37.86) 32 (31.07) 32 (31.07) |
| Employment (n = 103) |
100% <100% |
72 (69.9) 31 (30.1) |
|
| Type of shift (n = 103) |
Daytime Two-shift work Three-shift work Night shift |
2 (1.9) 23 (22.3) 65 (63.1) 13 (12.6) |
4.1 Descriptive Results of QPS Scales and Single Items
With respect to the area Job demands, the participants responded that in their work as CCNs, they sometimes faced quantitative demands and they rather often met decision demands. They rather often met positive challenges at work as CCNs. They reported that interruptions that disturb their work occur rather often (52%) or very often or always (18.6%). When it came to the area Control at work, they rather seldom had control of decisions about their daily work or control of work pace. Concerning the area Mastery of work, the CCNs stated that they rather often had perception of mastery.
The participants’ response to the single items is shown in Table 3. They seldom (26.2%) or sometimes (48.5%) got information about the quality of the work they did. Regarding Work motives, they considered both intrinsic and extrinsic motivation to work as rather important (Table 3).
| N | Median | Mean | SD | |
|---|---|---|---|---|
| Job demands1 | ||||
| Quantitative demands | 102 | 3.00 | 3.09 | 0.47 |
| Is your workload irregular so that the work piles up? | 100 | 3.00 | 3.00 | 0.74 |
| Do you have to work overtime? | 102 | 3.00 | 2.60 | 0.76 |
| Is it necessary to work at a rapid pace? | 102 | 4.00 | 3.71 | 0.67 |
| Do you have too much to do? | 102 | 3.00 | 3.05 | 0.71 |
| Decision demands | 102 | 4.00 | 4.05 | 0.50 |
| Does your work require quick decisions? | 102 | 4.00 | 3.99 | 0.68 |
| Does your work require maximum attention? | 102 | 5.00 | 4.51 | 0.63 |
| Does your work require complex decisions? | 102 | 4.00 | 3.64 | 0.82 |
| Learning demands | 103 | 3.00 | 2.84 | 0.54 |
| Are your work tasks too difficult for you? | 102 | 2.00 | 1.94 | 0.67 |
| Do you perform work tasks for which you need more training? | 102 | 2.00 | 2.46 | 0.82 |
| Does your job require that you acquire new knowledge and new skills? | 101 | 4.00 | 4.10 | 0.66 |
| Single items | ||||
| Does your work require physical endurance? | 102 | 4.00 | 3.54 | 0.85 |
| Does your work require great precision of movement? | 102 | 4.00 | 3.60 | 0.92 |
| Are there interruptions that disturb your work? | 102 | 4.00 | 3.86 | 0.73 |
| Is your work monotonous? | 102 | 2.00 | 1.94 | 0.76 |
| Do you have to repeat the same work procedure at intervals of a few minutes? | 102 | 3.00 | 2.56 | 0.92 |
| Is it possible to have social contact with co-workers while you are working? | 102 | 4.00 | 3.74 | 0.77 |
| Are errors in your work associated with a risk of personal injury? | 100 | 3.00 | 2.88 | 1.37 |
| Are errors in your work associated with the risk of economic losses? | 99 | 2.00 | 2.10 | 1.17 |
| Control at work1 | ||||
| Positive challenges at work | 103 | 4.00 | 4.41 | 0.44 |
| Are your skills and knowledge useful in your work? | 102 | 5.00 | 4.70 | 0.52 |
| Is your work challenging in a positive way? | 102 | 4.00 | 4.13 | 0.61 |
| Do you consider your work meaningful? | 102 | 4.00 | 4.41 | 0.59 |
| Control of decision | 103 | 2.40 | 2.44 | 0.49 |
| If there are alternative methods for doing your work- can you choose which method to use? | 103 | 3.00 | 3.45 | 0.67 |
| Can you influence the amount of work assigned to you? | 103 | 2.00 | 2.43 | 0.72 |
| Can you influence decisions concerning the persons you will need to collaborate with? | 103 | 2.00 | 1.71 | 0.76 |
| Can you decide when to be in contact with clients? (Patients and family)? | 102 | 1.00 | 1.64 | 0.94 |
| Can you influence decisions that are important for your work? | 102 | 3.00 | 2.94 | 0.82 |
| Control of work pace | 103 | 2.00 | 2.32 | 0.72 |
| Can you set your own work pace? | 103 | 3.00 | 2.70 | 0.82 |
| Can you decide yourself when you are going to take a break? | 103 | 3.00 | 2.89 | 0.96 |
| Can you decide the length of your break? | 103 | 2.00 | 1.86 | 0.94 |
| Can you set your own working hours (flexitime)? | 103 | 1.00 | 1.83 | 1.30 |
| Mastery of work1 | ||||
| Perception of mastery | 103 | 4.00 | 4.12 | 0.39 |
| Are you content with the quality of the work you do? | 103 | 4.00 | 4.14 | 0.49 |
| Are you content with the amount of work that you get done? | 103 | 4.00 | 3.99 | 0.51 |
| Are you content with your ability to solve problems at work? | 103 | 4.00 | 4.06 | 0.50 |
| Are you content with your ability to maintain a good relationship with your co-workers at work? | 103 | 4.00 | 4.29 | 0.54 |
| Single items | ||||
| Do you get information about the quality of the work you do? | 103 | 3.00 | 2.87 | 0.86 |
| Can you yourself immediately assess whether you did your work well? | 102 | 4.00 | 3.80 | 0.72 |
| Work motives2 | ||||
| Intrinsic motivation to work | 102 | 4.00 | 3.76 | 0.53 |
| How important are the following considerations in relation to your ideal job: | ||||
| To develop my own personality | 102 | 4.00 | 4.00 | 0.70 |
| To get a sense of accomplishing something worthwhile | 101 | 4.00 | 4.16 | 0.61 |
| To be able to put my imagination and creativity to good use at work | 101 | 4.00 | 3.13 | 0.85 |
| Extrinsic motivation to work | 102 | 4.00 | 3.93 | 0.51 |
| How important are the following considerations in relation to your ideal job: | ||||
| To have a peaceful and orderly job | 102 | 4.00 | 3.84 | 0.70 |
| That the work is secure and provides regular income | 102 | 4.00 | 4.20 | 0.69 |
| To have a safe and healthy physical work environment | 102 | 3.00 | 3.76 | 0.75 |
| Single items | ||||
| To have good pay and material benefits? | 102 | 4.00 | 3.79 | 0.78 |
1) 1 = very seldom or never 2 = rather seldom 3 = sometimes 4 = rather often 5 = very often or always
2) 1 = unimportant 2 = not so important 3 = rather important 4 = very important 5 = absolutely necessary
4.2 Subgroup Comparisons
Comparisons between subgroups of the CNN background variables were conducted with regard to the four area of QPS scales with single items. Significant differences between subgroups are displayed in Table 4. With respect to the area Job demands, the subgroup of CCNs with three shifts had the significantly highest score for the scale decision demand. Regarding the single items in the area, significant differences were found between age groups and years after postgraduate education. Concerning the area Mastery of work, the subgroup of CCNs with 6–14 years’ experience as a CCN after postgraduate education (n = 50) had the significant highest score on perception of mastery. With regard to the area Work motives, the age group ≥50 years (n = 37) had the highest mean score in the scale intrinsic motivation to work (see Table 4).
5 Discussion
The aim of the study was to investigate Norwegian CCNs’ psychological and social factors at work in an ICU. The following research questions were investigated: 1) How do CCNs perceive job demands, control at work, mastery of work and work motives related to their work in ICUs? 2) Is there any difference between CCNs’ perceptions of job demands, control at work, mastery of work and work motives regarding age, gender, years in present workplace, experience as a CCN and type of working shifts? The results of this study suggest that participants experienced high expectations regarding quantitative- and decision demands, but less control at work. They rather seldom or sometimes got information about the quality of the work they performed. Nevertheless, they found their work challenging in a positive way and experienced a strong sense of mastery. Some significance differences were found between CCNs’ type of shift, age, and years of experience as a CCN.
5.1 CCNs Perceptions of Job Demands and Control at Work
High scores may indicate that the CCNs rather often encountered demands for making decisions. Keeping in mind that CCNs’ work in ICUs is characterized by high-tech equipment and working with the most complex patients (1), this is understandable. They work with acute and critically ill patients in all age groups and have independent nursing responsibilities in their professional practice. Moreover, they are carrying out complex tasks. The work can include rapid and unpredictable changes where the patient’s health and safety depend on the quality of the job (1). According to the SEIPS model (27), health care systems such as ICUs can be conceptualized as work systems in which people perform multiple tasks using various tools and technologies in a physical environment and under specific organizational conditions. Those system interactions influence care processes and patient outcomes (27).
The results also pointed to the fact that the CCNs rather seldom experience having control of decisions and control of work pace. There are interruptions that disturb their work rather often. Several studies have found similar results with a high level of job demands combined with a lower level of control (28,29,30). High demands can be positive if followed by a high degree of control (21). Van Bogaert and Peremans (31) found that decision-making latitude had a stimulating impact on personal accomplishment and dedication for nurses working in acute care hospitals. High demands and low control, on the other hand, can lead to stress and subsequent health problems, burnout and sickness absence (7,8,30). Both low job satisfaction and a high level of job stress are correlated with high burnout scores among CCNs (32). A systematic review of the work environment in the Nordic countries showed that low control of the work situation, and the combination of high quantitative demands and low job control contribute to early retirement for Nordic employees (33). The combination of high demands and low control increases the risk of sickness absence, while control in itself together with a positive social climate reduces the risk of sickness absence (34).
| Area | Age | Experience as CCN after postgraduate education | Type of shifts | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kruskal-Wallis test | Kruskal-Wallis test | Kruskal-Wallis test | ||||||||||||
| Years (n) | Mean (SD) | X2 | P | Years | Mean (SD) | X2 | p | Years (n) | Mean (SD) | X2 | p | |||
| Job demand1) | N = 100 | 4.05 (0.50) | 12.89 | 0.01 | ||||||||||
| Decision demands (scale) | 2-shift (22) | 3.74 (0.50) | ||||||||||||
| 3-shift (65) | 4.16 (0.46) | |||||||||||||
| Nightshift (13) | 4.03 (0.44) | |||||||||||||
| Is it possible to have social | ≤ 35 (14) | 3.64 (0.75) | 10.65 | 0.01 | ||||||||||
| contact with co-workers while | 36–49 (51) | 3.98 (0.76) | ||||||||||||
| you are working? (single item) | ≥ 50 (36) | 3.44 (0.70) | ||||||||||||
| Are errors in your work | ≤ 35 (13) | 3.08 (1.26) | 10.89 | 0.00 | ≤ 5 (15) | 2.93 (1.53) | 9.46 | 0.01 | ||||||
| associated with a risk of personal | 36–49 (50) | 3.26 (1.32) | 6–15 (50) | 3.22 (1.25) | ||||||||||
| injury? (single item) | ≥ 50 (36) | 2.31 (1.30) | ≥ 15 (32) | 2.28 (1.30) | ||||||||||
| Are errors in your work | ≤ 35 (13) | 2.46 (1.33) | 9.13 | 0.01 | ≤ 5 (15) | 2.00 (1.25) | 10.55 | 0.01 | ||||||
| associated with the risk of | 36–49 (49) | 2.35 (1.22) | 6–15 (49) | 2.41 (1.21) | ||||||||||
| economic losses? (single item) | ≥ 50 (36) | 1.64 (0.90) | ≥ 15 (32) | 1.59 (0.91) | ||||||||||
| Mastery of work1)
Perception of mastery (scale) |
N = 100 | 4.12 (0.40) | 6.48 | 0.04 | ||||||||||
| ≤ 5 (17) | 4.04 (0.38) | |||||||||||||
| 6–15 (50) | 4.21 (0.34) | |||||||||||||
| ≥ 15 (33) | 4.02 (0.47) | |||||||||||||
| Work motives2)
Intrinsic motivation to work (scale) |
N = 101 | 3.76 (0.53) | 10.32 | 0.01 | ||||||||||
| ≤ 35 (14) | 3.55 (0.59) | |||||||||||||
| 36–49 (50) | 3.68 (0.54) | |||||||||||||
| ≥ 50 (37) | 3.96 (0.42) | |||||||||||||
1) 1 = very seldom or never 2 = rather seldom 3 = sometimes 4 = rather often 5 = very often or always
2) 1 = unimportant 2 = not so important 3 = rather important 4 = very important 5 = absolutely necessary
In our study, CCNs working a three shift schedule experienced decision demands significantly more often than those working a two shift schedule. Kwiatosz-Muc et al. (28) found that the most stressful circumstances for ICU workers included night shift and work overload, while age did not influence stress. A three shift schedule in ICUs leads to a heavy shift load, often with many night shifts. There are fewer CCNs at work during night shifts, which can lead to a more vulnerable situation and more patients to take care of. The doctor may not be present to any great extent, and several independent decisions must be made. Those with a two shift schedule more frequently have a day shift, which can lead to better staffing and greater opportunity for professional support. Nevertheless, the results indicated that the CCNs rather often experienced positive challenges at work.
5.2 CCNs Perceptions of Mastery of Work and Work Motives
The CCNs quite often experienced a fairly high degree of mastery. Mastery is closely related to control in that it gives confidence in one’s ability to carry out a task next time (21,35). The findings showed that the CCNs with 6–15 years of experience after postgraduate education, experienced mastery most often with the highest score. A more recent review found that demographics such as age and years of experience were predictors of compassion fatigue (25). Experience of coping depends on how one is able to meet requirements and is linked therefore to both requirements and control in the work (7). According to Benner and Have (36), nurses are “knowledgeable practitioners” after five years in the profession. They can see the totality of the situation and make decisions based on this. Several conditions can promote coping. Bandura (37) claims that it is possible to facilitate learning to perform a task well in advance, through mental preparation and automation. The belief in one’s own mastery is necessary to achieve a sense of control and gives an expectation of having action skills (38).
The results indicated that the participants rather seldom or sometimes get information about the quality of the work they performed. Recognition and social support are important and stimulating factors in terms of a good working environment and are related to motivation and coping (38). A study showed that greater social support from supervisors or colleagues decreased stress and fatigue (19). Social support is also closely linked to experience of requirements and control (23). There are many indications that it is important to be seen and appreciated regardless of age. According to CCNs, social support was one of the most important factors when considering whether to leave or stay in their present job (39). Lack of social support can lead to stress and is an important factor in respect of how nurses perform their work (40,41). Lack of social support from colleagues and supervisors was negatively associated with turnover (20). In addition to management’s awareness of factors such as support and frequent feedback to employees, increased support from colleagues may also be important. Research found that by focusing on teamwork when implementing a teamwork programme in a surgical ward, the teamwork skill “mutual support” contributed to the most comprehensive positive change in the ward culture (42).
A high average total score on motives may indicate that motivation is very important for the participants in relation to continuing in their present workplace. The findings showed that the oldest group of CCNs found intrinsic motivation significantly more important than the other groups. Intrinsic motivation is about getting a sense of accomplishment at work, among other factors (7). Motivation is related to mastery in that an experience of coping makes it possible for inner motivation to increase (37). The implementation of a Learning from excellence program in pediatric and neonatal ICUs tends to improve both self-confidence and the wellbeing of all caregivers (43). Focusing on teamwork skills and learning from excellence may be possible measures to improve the CCNs experience of control and mastery of work.
5.3 Limitations
Data collection dating back to 2016 may affect the timeliness of the result. However, there is limited research related to CCNs’ psychosocial working environment prior to the COVID-19 pandemic, and we therefore see the study results as a relevant contribution to the evidence base. The design of this study is based on a self-reported survey, which may lead to measurement bias (44). The relatively small response rate (42.9%) may also reduce the representativeness of the study population. The Cronbach’s alpha for the scales was somewhat lower than the QPSNordic validation study (45). Our study sample consisted of nurses only and had a smaller number of participants, which could explain the differences (44).
The participants were all employed in ICUs in urban areas. Although this sample may be relatively similar to samples from other regions, the findings must be generalized to other groups of CCNs with caution. The questionnaire QPSNordic is validated in the Norwegian language and has been adjusted to the Nordic countries (45). Issues such as the length of the instrument have been considered (46). Only four areas of the questionnaire were chosen based on common knowledge of the CCNs’ challenges at work, although this may be a limitation of the study. Leadership may influence the four areas, but this was not included as an area in this study.
6 Conclusions
In conclusion, our study suggests that the CCNs had somewhat varying perceptions of psychological and social factors related to their work in the ICU. These included job demands, control at work, mastery at work, and work motives. Although their work required quantitative and decision demands including quick decisions and maximum attention, they had control of decision making and work pace to a lesser extent. They rather seldom received information about the quality of the work they performed. Nevertheless, they found their work challenging in a positive way and experienced a strong sense of mastery. Subgroups comparison of CNNs’ background found some differences in their perceptions. In the light of the results in the current study, it is important to maintain focus on the CCNs’ psychological and social work factors in ICUs. Many of the ICUs are under pressure due to reorganization and increasing demands regarding efficiency. The CCNs working in these units also experienced a very challenging period during the COVID-19 pandemic (47). We especially recommend that future research on CCNs’ perceptions of psychological and social work factors focuses on working shifts, age and experiences. Furthermore, research on the relationship between leadership and the CCNs’ in creating a healthy ICU working environment may be warranted.
Acknowledgement
The authors would like to express their gratitude to the critical care nurses who participated in the study.
Conflict of interest
All authors declare that there is no conflict of interest
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Authorship
TS, SJ, and RB were responsible for the conception and study design. TS and SJ performed the data collection. TS, SJ and RB contributed to the analysis of the data. TS, SJ and RB were involved in drafting the manuscript and revising it critically for important intellectual content. All authors have read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author, [TS], upon reasonable request.
References
- 1. Urden L. Critical care nursing diagnosis and management. 8th ed. Stacy KM, ed. Missouri: Elsevier; 2017. p. 1–8.
- 2. Karanikola M, Mpouzika M. Time to create a healthy work environment in icu: a review of current evidence and commentary. Connect. 2018;12(2):44–7. https://doi.org/10.1891/1748-6254.12.2.44
- 3. Epp K. Burnout in critical care nurses: a literature review. Dynamics. 2012;23: 25–31. https://doi.org/10.1016/j.cnc.2019.07.008
- 4. van Mol MM, Kompanje EJ, Benoit DD, Bakker J, et al. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: a systematic review. PloS one, 2015;10(8):e0136955. https://doi.org/10.1371/journal.pone.0136955
- 5. Seierstad T, Eimot M. Rapport ABIO ressurs. Oslo: Analysesenteret; 2015.
- 6. Meld. St. 7 (2020–2023). National health and hospital plan 2020–2023. Oslo: Ministry of Health and Care Services; 2020.
- 7. Dallner M, Elo A-L, Gamberale F, Hottinen V, Knardahl S, et al. Validation of the General Nordic Questionnaire (QPSNordic) for psychological and social factors at work. København: Nordisk Ministerråd; 2000.
- 8. Lindstøm K, Elo A-L, Skogstad A, Dallner M, Gamberali F, et al. User’s guide for the QPS Nordic. General Nordic questionnaire for psychological and social factors at work. Copenhagen: Nordic Council of Ministers; 2000.
- 9. Karasek R, Theorell T. Healthy work: stress, productivity, and the reconstruction of working life. New York: Basic Books; 1990.
- 10. Drews FA. Human factors in critical care medical environments. Rev Hum Factors Ergon. 2013;8(1):103–48.
- 11. Berland A, Natvig GK, Gundersen D. Patient safety and job-related stress: a focus group study. Intensive Crit Care Nurs. 2008;24(2):90–7. https://doi.org/10.1016/j.iccn.2007.11.001
- 12. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994–1001. https://doi.org/10.1111/j.1365-2834.2009.01027.x
- 13. Stone PW, Mooney-Kane C, Larson EL, Horan T, Glance LG, et al. Nurse working conditions and patient safety outcomes. Med Care. 2007;45(6):571–8. https://doi.org/10.1097/MLR.0b013e3180383667
- 14. Khan N, Jackson D, Stayt L, Walthall H. Factors influencing nurses’ intentions to leave adult critical care settings. Nurs Crit Care. 2019;24–32. https://doi.org/10.1111/nicc.12348
- 15. Ma C, Olds DM, Dunton NE. Nurse work environment and quality of care by unit types: a cross-sectional study. Int J Nurs Stud. 2015;52(10):1565–72. https://doi.org/10.1016/j.ijnurstu.2015.05.011
- 16. Fiabane E, Giorgi I, Sguazzin C, Argentero P. Work engagement and occupational stress in nurses and other healthcare workers: the role of organisational and personal factors. J Clin Nurs. 2013;22(17–18):2614–24. https://doi.org/10.1111/jocn.12084
- 17. Ruiz-Dilig A, MacDonald I, Varin M, Vandyk A, Graham I, et al. Job satisfaction among critical care nurses: a systematic review. Pub Med Gov. 2018;88:123–34. https://doi.org/10.1016/j.ijnurstu.2018.08.014
- 18. Shoorideh FA, Ashktorab T, Yaghmaei F, Alavi Majd H. Relationship between ICU nurses’ moral distress with burnout and anticipated turnover. Nurs Ethics. 2015;22(1):64–76. https://doi.org/10.1177/0969733014534874
- 19. Jones G, Hocine M, Salomon J, Dab W, Temime L. Demographic and occupational predictors of stress and fatigue in French intensive-care registered nurses and nurses’ aides: a cross-sectional study. Int J Nurs Stud. 2015;52(1):250–9. https://doi.org/10.1016/j.ijnurstu.2014.07.015
- 20. Blake N, Leach LS, Robbins W, Pike N, Needleman J. Healthy work environments and staff nurse retention: the relationship between communication, collaboration, and leadership in the pediatric intensive care unit. Nurs Adm Q. 2013;37(4):356–70. https://doi.org/10.1097/NAQ.0b013e3182a2fa47
- 21. Daouda OS, Hocine MN, Temime L. Determinants of healthcare worker turnover in intensive care units: a micro-macro multilevel analysis. Plos One. 2021;16(5):e0251779. https://doi.org/10.1371/journal.pone.0251779
- 22. Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, et al. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11):1037–45. https://doi.org/10.1056/NEJMsa1001025
- 23. West E, Barron DN, Harrison D, Rafferty AM, Rowan K, et al. Nurse staffing, medical and mortality in intensive care: an observational study. Int J Nurs Stud. 2014;51(5):781–94. https://doi.org/10.1016/j.ijnurstu.2014.02.007
- 24. Friganović A, Selič P, Ilić B, Sedić B. Stress and burnout syndrome and their associations with coping and job satisfaction in critical care nurses: a literature review. Psychiatr Danub. 2019;31(Suppl 1):21–31. PMID: 30946714.
- 25. Sacco TL, Ciurzynski SM, Harvey ME, Ingersoll GL. Compassion satisfaction and compassion fatigue among critical care nurses. Crit Care Nurse. 2015;35(4):32–42. https://doi.org/10.4037/ccn2015392
- 26. Sykepleiernes samarbeid i Norden. Ethical guidelines for nursing research in the Nordic countries = Etiske retningslinjer for sykepleieforskning i Norden. Oslo: Sykepleiernes Samarbeid i Norden; 2003.
- 27. Carayon P, Hundt AS, Karsh BT, Gurses AP, Alvarado CJ, et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15(suppl 1):i50-i8. https://doi.org/10.1136/qshc.2005.015842
- 28. Kwiatosz-Muc M, Fijałkowska-Nestorowicz A, Fijałkowska M, Aftyka A, Kowalczyk M. Stress prevalence and stressors among anaesthesiology and intensive care unit workers: a multicentre survey study. Aust Crit Care. 2018;31(6):391–5. https://doi.org/10.1016/j.aucc.2017.11.001
- 29. Trousselard M, Dutheil F, Naughton G, Cosserant S, Amadon S, Dualé C, et al. Stress among nurses working in emergency, anesthesiology and intensive care units depends on qualification: a job demand-control survey. Int Arch Occup Environ Health. 2016;89(2):221–9. https://doi.org/10.1007/s00420-015-1065-7
- 30. Aagestad C, Tynes T, Sterud T, Johannesen H, Gravseth H, et al. Factbook om working environment and health 2015: status and trends. Oslo: Statens arbeidsmiljøinstitutt; 2015.
- 31. Van Bogaert P, Peremans L, Van Heusden D, Verspuy M, Kureckova V, et al. Predictors of burnout, work engagement and nurse reported job outcomes and quality of care: a mixed method study. BMC Nurs. 2017;16(1):5. https://doi.org/10.1186/s12912-016-0200-4
- 32. Myhren H, Ekeberg Ø, Stokland O. Job satisfaction and burnout among intensive care unit and physicians. Crit Care Res Pract. 2013;2013:786176–6. https://doi.org/10.1155/2013/786176
- 33. Knardahl S, Johannessen HA, Sterud T, Härmä M, Rugulies R, et al. The contribution from psychological, social, and organizational work factors to risk of disability retirement: a systematic review with meta-analyses. BMC Public Health. 2017;17(1):176. https://doi.org/10.1186/s12889-017-4059-4
- 34. Knardahl S, Sterud T, Birkeland M, Nordby K. Arbeidsplassen og sykefravær – arbeidsforhold av betydning for sykefravær. Tidsskrift for velferdsforskning. 2016;19:179–99.
- 35. Bakker AB, Demerouti E. The job demands-resources model: state of the art. J Manag Psychol. 2007;22(3):309–28. https://doi.org/10.4102/sajip.v37i2.97
- 36. Benner P, Have G. From novice to expert: skills and strength in clinical nursing practice. Oslo: Tano & Munksgaard; 1995.
- 37. Bandura A. Self-efficacy: the exercise of control. New York: Freeman; 1997.
- 38. Foss Ø. Work health: health book for working life. Oslo: Gyldendal arbeidsliv; 2012.
- 39. van Dam K, Meewis M, van der Heijden BIJM. Securing intensive care: towards a better understanding of intensive care nurses’ perceived work pressure and turnover intention. J Nurs. 2013;69(1):31–40. https://doi.org/10.1111/j.1365-2648.2012.05981.x
- 40. Emberland JS, Knardahl S. Contribution of psychological, social, and mechanical work to low ability: a prospective study. J Occup Environ Med. 2015;57(3):300–14. https://doi.org/10.1111/j.1365- 2648.2012.05981.x
- 41. Eklöf M, Törner M, Pousette A. Organizational and social-psychological conditions in healthcare and their importance for patient and staff safety. A critical incident study among doctors and nurses. Saf Sci. 2014;70:211–21. https://doi.org/10.1016/j.ssci.2014.06.007
- 42. Ballangrud R, Aase K, Vifladt A. Longitudinal team training programme in a Norwegian surgical ward: a qualitative study of nurses’ and physicians’ experiences with teamwork skills. BMJ Open. 2020;10(7):e035432-e. https://doi.org/10.1136/bmjopen-2019-035432
- 43. Breinig S, Pinot A, Pujol J, Ikhlef H, Blasy C, Marcoux MO. The “3R Team” in action! Implementation of a program of learning from excellence in a neonatal and pediatric intensive care unit in France. Arch Pediatr. 2022;29(3):225–9. https://doi.org/10.1016/j.arcped.2022.01.005
- 44. Polit DF, Beck CT. Essentials of nursing research: appraising evidence for nursing practice. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2014.
- 45. Lindström K, Dallner M, Elo A-L, Gamberale F, Knardahl S, et al. Review of psychological and social factors at work and suggestions for the general Nordic questionnaire (QPS Nordic): description of the conceptual and theoretical background of the topics selected for coverage by the Nordic questionnaire. Copenhagen: Nordic Council of Ministers; 1997.
- 46. Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practice. Philadelphia: Wolters Kluwer Health; 2012.
- 47. Gualano MR, Sinigaglia T, Lo Moro G, Rousset S, Cremona A, et al. The burden of burnout among healthcare professionals of intensive care units and emergency departments during the COVID-19 pandemic: a systematic review. Int J Environ Res Pub Health. 2021;18(15):8172. https://doi.org/10.3390/ijerph18158172
Vedlegg 1
STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies
| Item No | Recommendation | PageNo | |
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract |
v |
(b) Provide in the abstract an informative and balanced summary of what was done and what was found |
v | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 5–80 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 82–89 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 1, 2, 93, 94 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 98–102 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants |
518 tab.2 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | Tab 3,4 |
| Data sources/ measurement | 8* | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 127–137
Tab 3, 4 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 274–289 |
| Study size | 10 | Explain how the study size was arrived at | 98 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 127–132 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding |
127–137 |
(b) Describe any methods used to examine subgroups and interactions |
127–137 | ||
(c) Explain how missing data were addressed |
|||
(d) If applicable, describe analytical methods taking account of sampling strategy |
|||
(e) Describe any sensitivity analyses |
|||
| Results | |||
| Participants | 13* | (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed |
476 |
(b) Give reasons for non-participation at each stage |
476 | ||
(c) Consider use of a flow diagram |
476
Fig 1 |
||
| Descriptive data | 14* | (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders |
149–152 |
(b) Indicate number of participants with missing data for each variable of interest |
Not possible | ||
| Outcome data | 15* | Report numbers of outcome events or summary measures | Tab 3,4 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included |
137 |
(b) Report category boundaries when continuous variables were categorized |
Tab 3,4 | ||
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period |
|||
| Other analyses | 17 | Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses | 175 |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | Tab 3,4
189 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 273 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 189–271 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 11, 12 |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 317 |
*Give information separately for exposed and unexposed groups.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.